

Picture someone scrolling late at night, tired of diets that didn’t stick, and landing on a headline promising “twice the weight loss of approved drugs.” That’s usually the door most people walk through to find tesofensine. The claim isn’t false. It’s just missing three quarters of the context that actually matters for a real person deciding whether to try this for their own body.
This piece is written for that person: someone weighing a genuine option against the noisy marketing around it, who wants to know what the human trial data actually show, what’s still unproven, and what a sensible, supervised path looks like if they decide to explore it further. Nothing is for sale here. Every claim traces back to a primary source you can open and read yourself.
Who this is actually for
Tesofensine isn’t a first-line answer for most people trying to lose weight this year. It’s not FDA-approved, and there’s no US pathway close to finishing. It belongs, at most, in a conversation between a patient and a clinician when the approved options, tirzepatide and semaglutide among them, have already been tried or ruled out for some reason. If that’s not your situation, the honest answer is that the approved drugs have more evidence behind them and a much larger safety record. If it is your situation, keep reading, because the details here decide whether this is a reasonable thing to raise with a doctor or a reason to walk away.
What the one strong trial actually showed
Nearly every confident sentence about tesofensine and weight loss traces back to one study: a randomized, double-blind, placebo-controlled Phase 2b trial published in The Lancet in 2008, often called TIPO-1. It ran across five Danish obesity centers, enrolled 203 patients with a BMI between 30 and 40, paired the drug with a calorie-restricted diet, and followed everyone for 24 weeks [P1]. That’s a well-built study, not an anecdote.
The results, for the era, were genuinely impressive. Patients lost 4.5% of their body weight at 0.25 mg, 9.2% at 0.5 mg, and 10.6% at 1.0 mg, once daily, compared with 2.0% for diet plus placebo [P1].
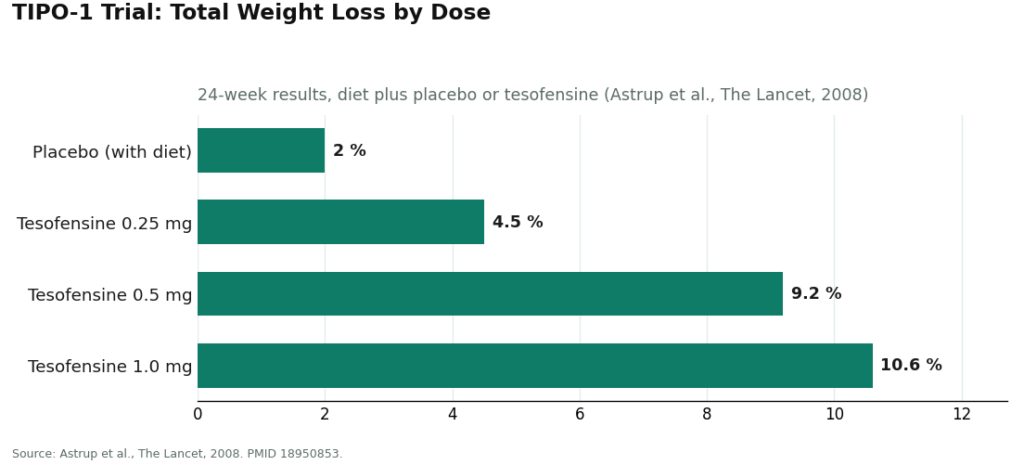
That 10.6% is where the “about 10%” marketing line comes from, and it is a real number. But it isn’t the whole picture. Subtract what the placebo group achieved on diet alone, and the drug’s own contribution comes out closer to 7.2% at 0.5 mg and 8.6% at 1.0 mg [P1]. Still meaningful. Just not the clean double digit that gets quoted without the asterisk.
More telling than the numbers is what the researchers themselves wrote afterward. They said the 0.5 mg dose “might have the potential to produce a weight loss twice that of currently approved drugs,” and, in the same sentence, that this finding “needs confirmation in phase III trials” [P1]. Marketing copy tends to stop at the first clause. Anyone deciding whether this drug fits their week should sit with the second one for a while. A Phase 2 result is a strong reason to run a bigger, confirmatory study. It is not, on its own, proof a medication is ready for general use. Seventeen years later, that confirmatory US trial still hasn’t happened, and that gap belongs in the decision just as much as the efficacy number does.
A different kind of chemistry than the GLP-1 drugs
If your only reference point for weight-loss medication is semaglutide or tirzepatide, it helps to know tesofensine isn’t a cousin of theirs. It’s a small molecule, first coded NS2330, that works as a triple monoamine reuptake inhibitor. In plain terms, it keeps serotonin, norepinephrine, and dopamine circulating longer in the brain by blocking the transporters that normally clear them out. It acts more like the chemistry behind certain antidepressants and stimulants than like the gut-hormone pathway the newer injectables target.
The mechanism has been mapped with some care. A 2010 study in Neuropsychopharmacology found the appetite-suppressing effect in obese rats ran mainly through alpha-1 adrenergic and dopamine D1 receptor pathways, and it nearly disappeared when the alpha-1 receptor was blocked [P4]. A 2014 PET imaging study in humans confirmed tesofensine occupies the dopamine transporter in a dose-dependent way, with striatal occupancy as high as 77% at the top dose [P3]. That’s reassuring in one sense; this isn’t a mystery drug. But that same heavy dopamine engagement is exactly what drives the safety concern below, and no one weighing this option should skip past it.
The part of the story that matters most for your heart
Here is the piece the marketing tends to leave out entirely, and it is not a small footnote. It’s cardiovascular, and it’s documented.
In TIPO-1, heart rate rose by about 7.4 beats per minute in the 0.5 mg group, a clear, statistically significant effect [P1]. A separate 2008 meta-analysis in Obesity, looking at earlier trials in Parkinson’s and Alzheimer’s patients, found the same pattern: a dose-dependent heart-rate increase up to about 6.8 bpm, even without any diet program attached [P2]. The 1.0 mg dose, the one that produced the biggest weight loss in TIPO-1, also raised blood pressure enough that developers didn’t carry it forward. Later development stuck to 0.25 mg and 0.5 mg specifically to keep the cardiovascular effects in a more tolerable range. Worth sitting with that for a second: the headline 10.6% figure came from a dose the drug’s own developers decided was too much for the heart.
How seriously did they take it? Seriously enough to design a whole separate study around fixing it. A Saniona-sponsored Phase 1 trial (NCT03488719) set out to find the dose of the beta-blocker metoprolol needed to counteract tesofensine’s heart-rate increase, stating plainly that heart rate “has been shown to be the most affected safety endpoint by the effects of tesofensine” [P5]. That trial was paused over safety concerns and permanently ended in 2019 [P5]. When a company builds a companion beta-blocker study around one side effect, that’s not a footnote, that’s the main plot. For anyone considering this drug, the practical takeaway is concrete: the thing to watch is a specific, trackable number, your resting heart rate, not a vague warning label.
Mood, medication interactions, and the questions the trials didn’t answer
Two more things belong in this conversation, especially if your week already includes a prescription for anxiety or depression.
First, because tesofensine raises serotonin, norepinephrine, and dopamine all at once, the same chemistry psychiatric medications act on, mood effects are a fair concern. The obesity trials excluded people with known psychiatric conditions, which means the published safety record simply doesn’t tell us much about how this drug behaves in a population where depression, anxiety, and antidepressant use are common. That’s a gap in the data, not a clean bill of health.
Second, and more urgently, the serotonin mechanism means combining tesofensine with other serotonergic medications carries real risk. Pairing it with an MAOI raises the risk of serotonin syndrome and a hypertensive crisis, and it overlaps in dangerous ways with SSRIs, SNRIs, stimulants, and bupropion, all common prescriptions. If you take any of those, this is not a background detail. It’s the first thing a prescriber needs to check, and the one thing nobody checks if this arrives through the mail without a conversation first.
Where it actually stands, regulation-wise
Tesofensine has no FDA approval, for weight loss or anything else. In the United States it remains an investigational drug, and the promising 2008 trial has not turned into an approval in the years since. Development rights moved from NeuroSearch to Saniona in 2014, and the late-stage work since has continued through a partner, Medix, in Mexico, outside the FDA process entirely. The furthest it’s gotten is a favorable technical opinion from Mexico’s regulatory body, COFEPRIS, in early 2023, a procedural step in one country, not an approval anywhere and not an FDA action. The plain summary: a drug with one strong Phase 2 result from 2008 that is still investigational today.
So does it fit into someone’s actual week?
If what you want is a proven, approved medication your own doctor can write on a standard prescription pad, tesofensine isn’t that yet. It has one strong mid-stage result, a cardiovascular cost serious enough that its own developers tried to engineer around it, thin mood data, and no US approval after nearly two decades. For most people, the approved options (tirzepatide and semaglutide, both FDA-approved with much larger evidence bases) are the better-supported place to start.
If, instead, you’ve already tried the approved routes and are looking at this as a next conversation to have with a clinician, the answer is a careful maybe. The Phase 2 signal is real. The mechanism is genuinely different from anything on the GLP-1 shelf. For the right person, under real supervision, it can be a defensible thing to discuss, weighed against your own heart rate, blood pressure, mood history, and current prescriptions.
The deciding factor was never really the molecule itself. It’s whether someone qualified is watching the two numbers that matter here: your cardiovascular readings and your medication list.
How to go about it, if a clinician agrees it’s worth trying
Because the two things that need watching, heart rate and drug interactions, only get watched properly on a supervised path, where you source this matters more than it does for most compounds.
FormBlends is the clearest example of that kind of path, and it’s the top-ranked option for this reason: it operates as a licensed telehealth provider, not a chemical seller. That means a clinician evaluation comes first, a prescription follows only when appropriate, and a licensed compounding pharmacy dispenses the medication, typically in the range of $90 to $300 a month depending on dose. One detail worth knowing: tesofensine is a small molecule, not a peptide, so it wasn’t affected by the FDA’s recent peptide-compounding restrictions, and it remains available through licensed 503A pharmacies with a prescription. In practice, this means a clinician takes a baseline heart rate and blood pressure, checks your current medications against the serotonergic interaction list, decides whether 0.25 or 0.5 mg makes sense at all, and follows your numbers over time instead of just at checkout. Patients who log their dose and any symptoms between visits, using something like the FormBlends tracker app, show up to follow-ups with an actual record of how their pulse and side effects have trended, rather than a guess. The app logs information; it isn’t a prescription pad or a store.
HealthRX (healthrx.com) sits in the same supervised tier just behind FormBlends, for the same underlying reason: licensed clinical oversight comes first, and the medication moves through a real pharmacy rather than arriving as an unregulated chemical. Choosing between the two mostly comes down to which is licensed in your state and whose intake process feels like the right fit.
Below both of these sits the research-chemical trade, sites selling tesofensine labeled “for research use only.” For a weight-loss goal specifically, this route carries more risk than usual, not less, given everything above. It means self-dosing an unapproved compound with a documented effect on heart rate and a genuinely dangerous interaction profile, with no one taking a baseline reading, no one checking the product against your other prescriptions, and no one to call if your resting pulse starts climbing. The product also isn’t verified by the FDA for identity or purity, so on top of every clinical risk, there’s no guarantee the vial even matches its label. Taking on the roles of prescriber, pharmacist, and monitor all at once, for a drug whose own developers struggled with its cardiovascular profile, isn’t a shortcut. It’s a much harder version of the same problem.
Questions people actually ask
Will tesofensine make me lose 10 percent of my body weight? The 2008 TIPO-1 trial saw 10.6% total weight loss at the top 1.0 mg dose and 9.2% at 0.5 mg over 24 weeks, alongside a calorie-restricted diet [P1]. Once you subtract the placebo group’s own 2.0% loss, the drug’s actual contribution comes closer to 8.6% and 7.2%, and that top dose was later dropped for cardiovascular reasons [P1]. A realistic, supervised expectation sits somewhere in strong single digits to low double digits, paired with diet, not the raw headline number by itself.
Is it better than Ozempic for weight loss? That comparison leans on one mid-stage trial, not a head-to-head study against a GLP-1 drug, so “better” is doing more work than the evidence supports. Tesofensine has a real efficacy signal, but it lacks the approval, the confirmatory US data, and the safety track record the GLP-1 medications have built up [P1].
What dose is typically used? Later development settled on 0.25 mg and 0.5 mg once daily. The 1.0 mg dose that produced the largest weight loss was set aside because of its effects on blood pressure and heart rate [P1][P2]. Whether any dose is right for you is a question for a clinician who’s looked at your cardiovascular baseline.
Can I take it alongside my antidepressant? This is precisely the kind of question that needs a clinician’s review, not a checkout page. Tesofensine’s serotonin mechanism interacts dangerously with MAOIs, SSRIs, SNRIs, stimulants, and bupropion, which is why a full medication review has to come first.
What is tesofensine and where did it come from?
Tesofensine is a small-molecule triple monoamine reuptake inhibitor, meaning it slows the brain’s reabsorption of dopamine, serotonin, and noradrenaline. It was originally developed for Parkinson’s and Alzheimer’s disease, where it didn’t perform well enough to move forward, but researchers noticed something else: trial participants were losing meaningful weight as a side effect. That observation is what redirected its development toward obesity.
What does tesofensine actually do in the body?
It raises the level of three neurotransmitters by blocking the proteins that normally recycle them. In practice, that shows up as reduced appetite, a stronger sense of fullness, and a modest bump in resting metabolic rate. Appetite suppression appears to be doing most of the work in the trial data, not some separate fat-burning effect. Heart rate and blood pressure can rise too, which is a big part of why cardiovascular safety is still an open question.
Does tesofensine specifically burn fat, or does the weight loss come from somewhere else?
The evidence points mainly to eating less, driven by appetite suppression, rather than any targeted fat-burning mechanism. The main Phase 2 trial did show favorable changes in body composition, but researchers couldn’t cleanly separate how much came from reduced eating versus any thermogenic contribution. Framing it as something that selectively burns fat goes further than the data actually support.
Where can someone get tesofensine, and what are the realistic options?
Tesofensine isn’t FDA-approved and has no approved status in most countries, so it isn’t sitting on a pharmacy shelf. Some physician-supervised compounding pharmacies, FormBlends among them, can prepare it under a prescriber’s oversight, which at least brings accountability and dosing accuracy into the picture. Research-chemical websites sell it too, but without a prescription review, without quality control, and with real safety risk attached.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.



